Diagnostic Tests of Motor Function
Spiral Analysis
Spiral Analysis is a non-invasive system of quantifying upper limb motor function based on kinematic and physiologic features derived from handwritten spirals. Spiral Analysis uses a digitizing tablet and writing pen connected to a computer to record position, force, and time measurements. No wires are attached and no needles are used. Spiral Analysis is patented under US # 6,454,706 entitled “System and Method for Clinically Assessing Motor Function.”
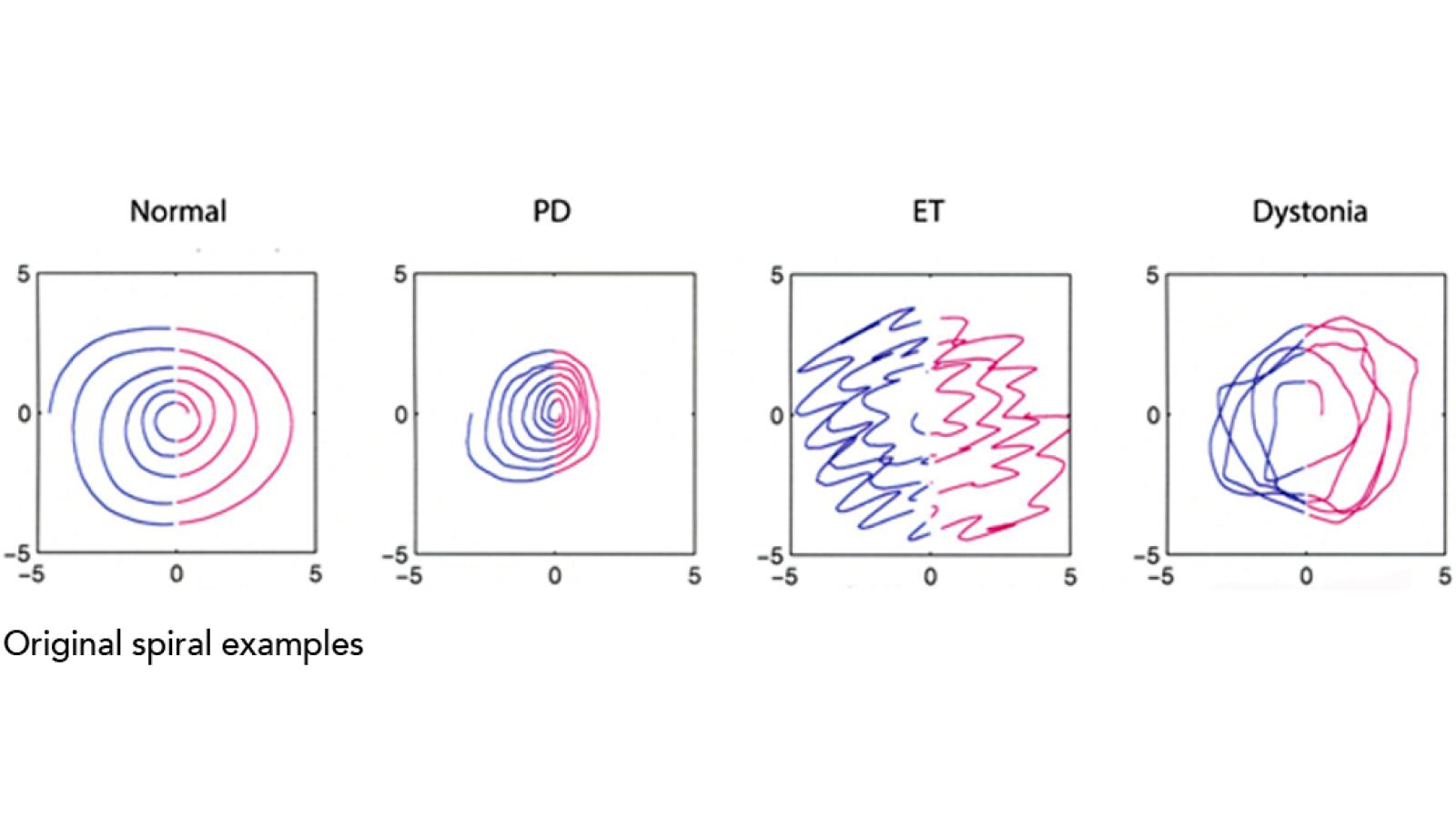
The test is based on “unraveling” the two-dimensional drawn spiral picture into a data series that captures its original kinematic information and allows for further computational manipulations and clinical correlations. Spiral data are collected in the X, Y, and pressure axes providing virtual “tri-axial” recordings. This effectively extends spiral drawing – a standard neurologic clinical test – into an objective and accurate measure of motor control. Output consists of a large spreadsheet array in text format as well as graphic displays. Mathematical formulations are developed into indices that quantify the kinematic parameters and assess many spiral features including shape, drawing speed, tightness of loops, irregularity, and tremor. Over 40 indices are created, and multiple spirals can be averaged.
Spiral Analysis provides greater accuracy and objectivity than the clinical exam alone. It can be used to study the details of normal motor control, quantify normal and abnormal motor development, and analyze movement disorders such as Parkinson’s disease, tremor disorders, or dystonia. Spiral Analysis is also useful in quantifying changes before and after a medical or surgical intervention such as deep brain stimulator implantation. Ongoing research is determining how helpful Spiral Analysis may be in diagnosing neurologic conditions and in early detection of disorders such as Parkinson’s disease.
Spiral Analysis Examples:
Tremor Analysis
Tremor analysis uses computers and special hardware to record important characteristics of tremors and other involuntary movements. This test determines the size and frequency of any type of tremor, and finds which muscles are most involved in causing tremors.
Side-to-side relationships between tremor movements and muscles are also examined. Special sensors called accelerometers register tremor movements. Muscle activity is recorded using surface electromyography (EMG) electrodes. Just as in the clinical examination, tremors are evaluated at rest and while the patient performs those tasks which bringout the tremors. Any region of the body (the arms, legs, head, etc) can be measured accurately and reproducibly with tremor analysis. An average test records data from at least two, often all four limbs, the head and neck, and takes 1-2 hours to complete.
Tremor analysis complements the clinical evaluation with objective and quantitative data that can be analyzed after the test is completed. Difficult medical diagnoses can be confirmed or excluded on the basis of this test. Certain tremors, such as orthostatic tremor, are definitively established using tremor analysis. The test is also useful in establishing baseline measurements for later comparison after different types of therapy. Important effects of medication, physical therapy or surgery can be assessed quantitatively.
EMG Profile Analysis (Polymyography)
This is a multi-channel electromyography (EMG) study used to record complex motor activity such as muscle firing patterns, activation order, agonist/antagonist relationships, reflexes, EMG recruitment profiles and EMG to action relationships. Continuous EMG signals and along with some accelerometry recordings are obtained simultaneously after which selected portions of the acquired data are superimposed, averaged, demodulated, integrated or analyzed with various Fourier transforms. Surface accelerometric and EMG electrodes are placed over selected body regions and the patient is recorded at rest and during specified activity. The testing procedure requires 30 minutes to 2 hours to perform depending on the complexity of the clinical syndrome.
EMG profile analysis is used to find the focus of movement onset and pattern of EMG activity in complicated movement disorders where muscle groups in multiple face and neck regions, several limbs, and/or the trunk are involved. Dystonia, spinal myoclonus, complex tics, startle syndromes and unusual tremors are conditions where the EMG and limb activity are most effectively recorded and analyzed with this technique.
Reaction Time and Movement Time Analysis
This is a psychophysical test measuring cognitive and motor function. It measures the ability to get ready to move (the reaction time) and the execution of the movement itself (the movement time). The hands and feet can be tested equally well. Instructional cues from a computer display tell patients about the direction and type of movement to be recorded. Cues and targets are presented on a computer monitor. Several trials involving different instructions on how to move, when, and in which direction, are presented to patients while they are seated comfortably. The test takes from 30 minutes to 1 hour depending on how many psychological issues are studied.
Reaction and movement times are among the useful measures of mental and motor function in neurologic conditions such as Parkinson’s disease and related disorders. Results from this test directly correlate with standard clinical scales of mental and motor function and can detect accurately the effects of medication or other therapy. Reaction and movement time measure sub-clinical brain processes that can reflect disease severity or treatment effect.
Backaveraging EEG to EMG
This is a study utilizing both electroencephalography (EEG) and electromyography (EMG). Portions of the EEG are averaged relative to involuntary muscle activity as measured by EMG. Backaveraging determines whether there are cortical potentials preceding involuntary movements that are time-locked to the EMG, providing strong evidence that the abnormal movements originate in higher centers of the brain such as the cerebral cortex. An EMG electrode on the appropriate muscle serves as a trigger for averaging cortical potentials recorded over the scalp. The patient is tested at rest, during movement-inducing maneuvers, or while subjected to visual, audio, or tactile stimuli. The test is usually completed in 2-3 hours and is often interpreted in conjunction with a standard EEG and somatosensory evoked potentials.
Backaveraging is a test of particular importance in several movement disorders where the origin of an abnormal movement is unclear, and therapy depends on the anatomic location of the disease. Usually, fast involuntary movements, such as myoclonic jerks, qualify for investigation with back averaging because of the importance of determining whether the origin of the muscle activity is in the cerebral cortex or lower in the nervous system (the brainstem or spinal cord). Additional types of quick involuntary movements, such as tics, chorea, and dystonia may be investigated with back averaging to rule out conditions that may implicate higher centers in the brain. The information contained in back averaging cannot be obtained during a routine EEG, even with a muscle recording electrode, because standard EEG does not employ signal averaging or backward time measurements.